UNDIFFERENTIATED PLEOMORPHIC SARCOMA - MALIGNANT FIBROUS HISTIOCYTOMA
- Hits: 618
Undifferentiated pleomorphic sarcoma is the most common malignant soft tissue tumor. It is also known as malignant fibrous histiocytoma. The exact cause and tissue of origin are unknown.
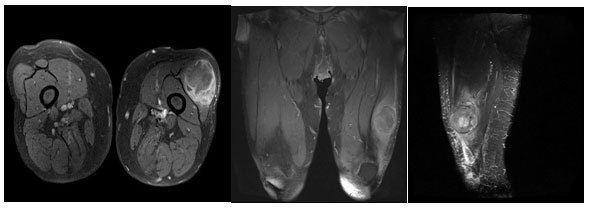
Undifferentiated pleomorphic sarcoma often occurs after age 40 (50-70) and in the thigh. It is slightly more common in males.
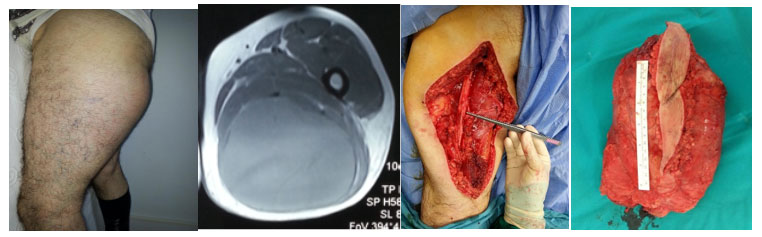
Patients with undifferentiated pleomorphic sarcoma often present to the doctor with a complaint of swelling. It is noted that the swelling increases with time. Pain is very rare. The fact that the swelling has been present for a long time and is painless may mislead the patient and the physician that it is benign.
The tumor is usually deep (90%) and large (>5cm). However, it can rarely be small and superficial. Similarly, a superficial and small tumor may mislead the patient and the physician.
Physical examination of patients with undifferentiated pleomorphic sarcoma usually reveals a soft, mobile, painless swelling. In patients who have waited a long time, the tumor may sometimes break through the skin.

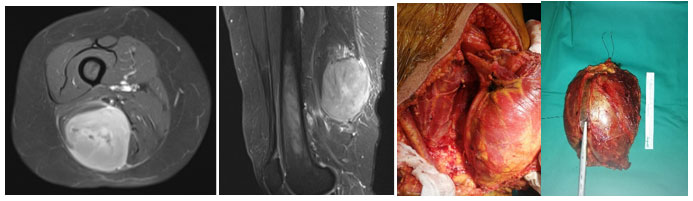
In patients with undifferentiated pleomorphic sarcoma, we most often use MRI with medication as the imaging method. MRI gives us detailed information about the location, size, borders, and contents of the tumor. MRI is also used to plan surgery, assess response to chemotherapy and radiation, and monitor for recurrence.
The definitive diagnosis of undifferentiated pleomorphic sarcoma is made by biopsy after clinical and radiologic evaluation. Biopsy is often performed using a closed procedure with special needles. It is important that the physician performing the biopsy is an orthopedic oncologist who specializes in bone and soft tissue tumor surgery and that the physician performing the microscopic examination is a specialist in bone and soft tissue pathology.

Patients diagnosed with undifferentiated pleomorphic sarcoma will undergo a CT scan or PET-CT to look for metastases (often hematogenous to the lungs).
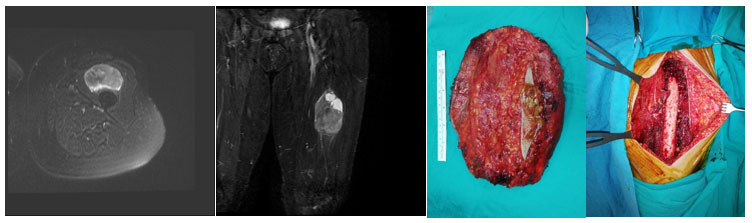
The main treatment for undifferentiated pleomorphic sarcoma is clean surgical removal of the tumor. The tumor that is not removed cleanly with wide margins has a nearly one hundred percent recurrence rate and is prone to metastasis. For this reason, it is important that the surgeon performing the surgery is an orthopedic oncologist with experience in this area.
Radiation therapy is used before or after surgery to facilitate surgery and reduce the possibility of recurrence. Although there are advantages and disadvantages of radiotherapy before or after surgery, there is no absolute superiority of one over the other.
Chemotherapy is not routinely used for undifferentiated pleomorphic sarcoma. Chemotherapy is used especially in the presence of metastases (often to the lungs) and in large and deep-seated tumors.
The five-year survival rate for patients with undifferentiated pleomorphic sarcoma is 60-65%. Life expectancy is lower for deep-seated and large tumors, especially in the presence of metastases.
Patients diagnosed with undifferentiated pleomorphic sarcoma should be followed for many years at regular intervals for recurrence and metastasis, which means spread to other parts of the body.
