POST-RADIATION SARCOMA
- Hits: 725
Post-radiation sarcoma is a late complication of radiation therapy. Although radiation therapy is used to treat many cancers, radiation-induced cancer is very rare.
Post-radiation sarcoma is common in patients receiving radiation therapy for gynecological (cervical, endometrial, etc.), gastrointestinal, breast, testicular, and prostate cancers. It also occurs in patients undergoing radiation therapy for Ewing sarcoma and soft tissue sarcoma.
Post-radiation sarcoma most commonly occurs in the pelvis, shoulder blade (scapula), ribs, clavicle and spine.
The risk of post-radiation sarcoma is higher in patients who received radiation therapy during childhood.
Post-radiation sarcoma occurs on average 10-15 (3-33) years after radiotherapy. There is a 5-10% risk of developing over a 20-year period.
Post-radiation sarcoma is usually caused by high-dose (40-60 Gy) radiotherapy.
Concurrent chemotherapy (especially alkaline agents) increases the risk.
Severe pain and rapidly increasing swelling, initially intermittent and then constant, are the most common findings in patients with post-radiation sarcoma. Pathologic fracture may occur.
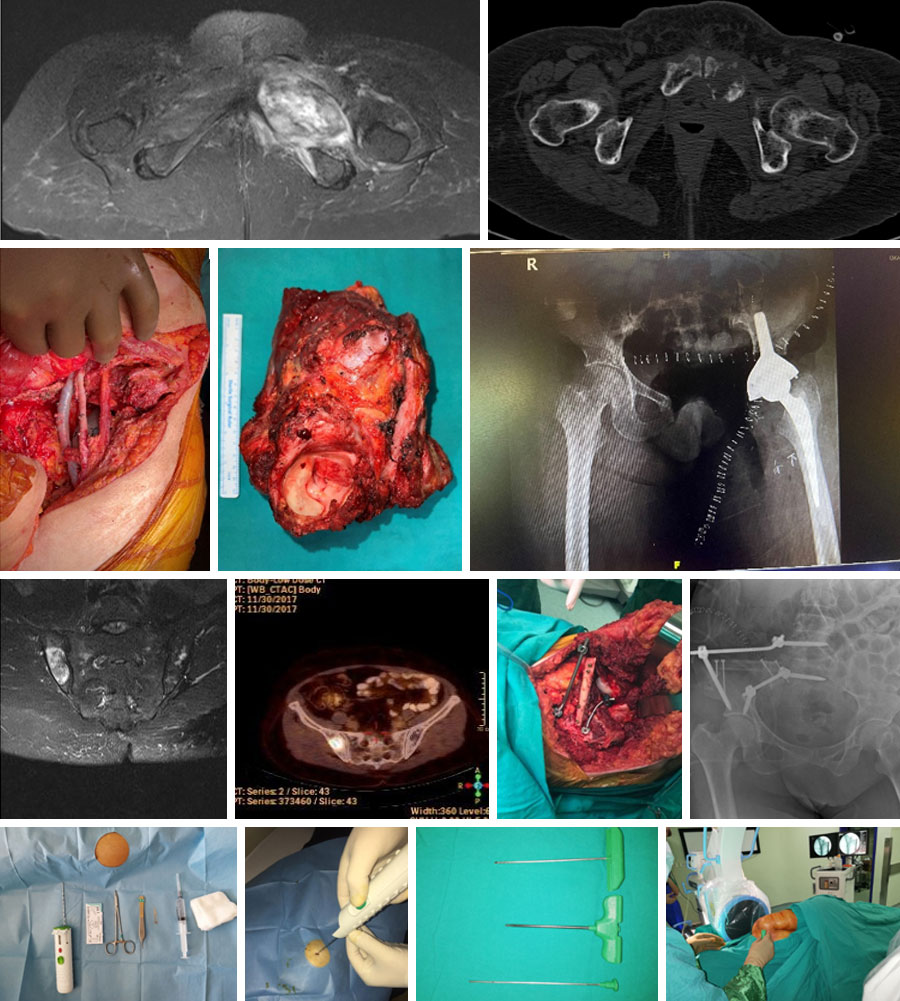
A soft tissue mass may accompany a lytic, aggressive, destructive bone lesion on radiologic studies of post-radiation sarcoma.
The definitive diagnosis of post-radiation sarcoma is made by biopsy and pathological evaluation often reveals high-grade sarcoma (bone: osteosarcoma, undifferentiated pleomorphic sarcoma, fibrosarcoma and chondrosarcoma. Soft tissue: angiosarcoma and leiomyosarcoma, etc.). It is important that the physician performing the biopsy is an orthopedic oncologist who specializes in bone and soft tissue tumors, and that the pathologist evaluating the biopsy sample is experienced in this area.
After the diagnosis of post-radiation sarcoma is confirmed by biopsy, screening for metastases (CT scan, PET-CT, etc.) is performed.
In the treatment of post-radiation sarcoma, clean removal of the tumor (wide resection) is extremely important, and amputation (removal of the limb) may be used for this purpose. Tumors that are not cleanly removed with wide margins have a nearly one hundred percent recurrence rate and are prone to metastasis. For this reason, it is essential that the surgeon performing the operation is an orthopedic oncologist with experience in this field.
Chemotherapy can be administered before or after surgery, but its effectiveness is low. Radiotherapy can be applied in selected cases.
Unfortunately, the prognosis for patients with post-radiation sarcoma is poor (5-year survival 11-48%). The risk of recurrence (17-68%) and metastasis (often to the lungs) is high. Clean surgical removal of the tumor is extremely important for survival. The prognosis is worse in cases of delayed diagnosis, large tumor that cannot be surgically removed cleanly, advanced age, anaplastic tumor, failure of adjuvant therapy.