CHORDOMA
- Hits: 1414
Chordoma is a malignant and slowly progressive tumor that develops from the notochord remnants of the bone. Chordoma usually occurs after the age of 40. There is no gender difference. It is located in the spine, most commonly in the neck (cervical vertebrae) and coccyx (sacrum).
Although pain is the most common complaint, patients may present with neurological complaints such as constipation in those with coccygeal localization, numbness and weakness in those with localization elsewhere in the spine. Patients with coccygeal localization may have difficulty sitting.
Because of the slow progression of chordoma and vague symptoms, there may be a delay in diagnosis.
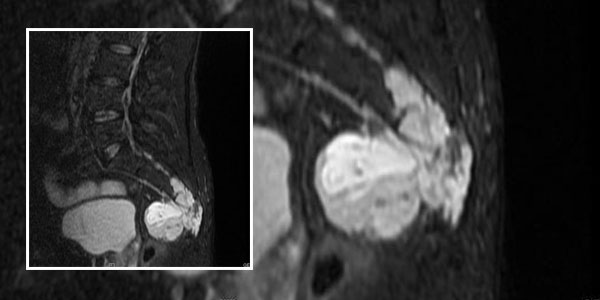
Radiologic evaluation of patients with suspected chordoma begins with plain radiography. The tumor may be missed on direct radiography because of intestinal gases. Tomography evaluates bone destruction in more detail. MRI shows the soft tissue component and the boundaries of the tumor in detail and is routinely performed with contrast. It also helps us plan surgery.
There is no significant value in laboratory tests of patients with chordoma.
After clinical and radiologic evaluation of the patient with suspected chordoma, the diagnosis is made by biopsy. We often prefer a closed needle biopsy. It is important that the physician performing the biopsy is an orthopedic oncologist specializing in bone and soft tissue tumor surgery and that the microscopic examination is performed by a physician specializing in bone and soft tissue pathology.
The patient diagnosed with chordoma should undergo a CT scan of the lungs for staging. Other parts of the spine should also be scanned with MRI for a second focus. PET-CT may also be performed for screening purposes.
Since chordoma is resistant to chemotherapy and radiotherapy, the main treatment is surgical removal of the tumor cleanly in one piece. The tumor that is not removed cleanly with wide margins has a nearly one hundred percent recurrence rate and is prone to metastasis. For this reason, it is important that the surgeon performing the surgery is an orthopedic oncologist with experience in this area. Depending on the location and size of the tumor, surgery may be performed from the back only, or surgical treatment may be performed by opening from both the front and back. Depending on the degree of sacral nerve root involvement, patients may experience problems with urination and defecation after surgery. For this reason, a colostomy (connecting the end of the intestine to a pouch in the abdomen) may be opened during surgery. The success of the first surgery is critical.
In cases of chordoma that cannot be removed cleanly, carbon ion or proton therapy can be applied, but unfortunately these treatments are not available in our country.
Chemotherapy has no place in the routine treatment of chordoma, but may be used in patients with dedifferentiated chordoma. Targeted drugs may be used in the presence of recurrence and metastasis.
Reconstruction for soft tissue coverage is essential, especially in cases of coccygeal chordoma, as the risk of postoperative wound problems is high.
Patients should be closely monitored because of the high risk of postoperative recurrence of chordoma and the possibility of metastasis to the lung.