BONE METASTASIS
- Hits: 565
Bone metastases is the spread of cancer from the organ of origin to the bone via the immediate environment, blood (often), or lymph. Venous Tumors/Metastases is more common than arterial Tumors/Metastases. Breast, prostate, and testicular Tumors/Metastases mostly spread by lymphatic route.
It is the most common malignant tumor of bone. It is often seen after the age of 40. Bone Tumors/Metastases indicates that the existing cancer is advanced. These patients should be evaluated in a multidisciplinary fashion (oncology, pathology, radiology, nuclear medicine, and orthopedic oncology).
In recent years, in parallel with the development of cancer therapies, the incidence of metastatic bone cancer has increased as life expectancy has increased. Bone is the third most common site of Tumors/Metastases after lung and liver. Depending on the type of cancer, 20-70% of all cancers metastasize to bone.


Patients with bone metastases can present to the clinic in many different ways. It may be the first sign of an advanced cancer, or it may be the Tumors/Metastases of a cured cancer that occurs years later. It may be detected during routine screening of the cancer patient without complaint, or the patient may present with a fracture due to direct weakening of the bone by the Tumors/Metastases.
Patients with bone metastases often present to the physician with pain. Typically, the pain is present at rest and increases in intensity over time. The patient may wake at night because of the pain and may not benefit from standard pain medications. Sometimes it is found during routine screening of patients with cancer when there are no complaints. Some patients are diagnosed with direct bone metastases despite having no history of cancer. In this case, life expectancy is shorter. Rarely (10-30%), the patient comes to the emergency room with a fracture caused by the Tumors/Metastases weakening the bone.
All cancers can metastasize to bone, but breast, prostate, lung, kidney, and thyroid cancers are the most common. This is because these cancers are more common in the population and patients with these cancers have a longer life expectancy.
Bone metastases are most commonly found in the spine, pelvis, femur, and humerus. Metastases may be single or multiple and may be lytic, sclerotic, or mixed, depending on the tissue of origin.
The diagnosis of bone metastases is critical, particularly in determining that the tumors do not originate from the bone itself and that they do not originate from a site other than the patient’s existing tumor. Failure to do so could lead to irreversible errors that could have a serious negative impact on the patient’s life. For this purpose, a biopsy may be necessary in some cases, after a detailed review of the patient’s history and physical examination, as well as the necessary radiologic studies. A two-dimensional x-ray of the entire affected bone is the most basic examination. Although tomography gives a better idea of bone destruction, patients with metastases of unknown origin will have lung and abdominal tomography to try to identify the cancer focus. MRI with medication is the best method for evaluating soft tissue. MRI also helps us plan surgery. If the patient does not have a history of cancer, or if a nuclear medicine scan (PET_CT or scintigraphy) of a patient with a history of cancer shows a single bone involvement, a biopsy is necessary. However, in 3-4% of patients, the origin of the tumor may not be identified.
If we suspect Tumors/Metastases in bone lesions detected especially in patients over 40 years of age, ESR and CRP tests are requested for the differentiation of infection; PSA, CEA, CA19-9, CA125, CA15-3, THYROGLOBULIN, Beta HCG, AFP, IMMUNOELECTROPHORESIS tests are requested for the detection of cancer.
The goal of treating bone metastases is to reduce pain, prevent fractures, and improve the patient’s function/quality of life. The type and extent of the tumor, the size of bone destruction, the response of the tumor to radiation therapy and chemotherapy, the general condition and life expectancy of the patient are the main factors in deciding the treatment. Treatment can be divided into two main categories: medical (bone-strengthening bisphosphonates, radiotherapy, chemotherapy, hormonotherapy, smart drugs) and surgical. Surgical treatment is used primarily in the presence or risk of fracture. Depending on the patient’s condition, closed (minimally invasive) or open methods may be preferred.
Early diagnosis and intervention is critical, as fracture development due to bone Tumors/Metastases will negatively impact the patient’s life expectancy. Intervention before fracture development reduces the risk of surgery, accelerates the patient’s return to daily activities, and reduces the need for additional surgery. In cases of fractures due to bone metastases, fixation (nail or plate) may be used or the tumor bone may be removed and replaced with a prosthesis. The patient should be carefully evaluated before making this decision. The method used should last for the remainder of the patient’s life and should not require reoperation.
Answers to the 7 Most Asked Questions about Bone Metastases
- What is bone Tumors/Metastases and how it develops
Bone Tumors/Metastases is the spread of cancer from the organ of origin to the bone via the immediate environment, blood (often), or lymph. Venous Tumors/Metastases is more common than arterial Tumors/Metastases. Breast, prostate, and testicular metastases mostly spread by lymphatic route. It is the most common malignant tumor of bone. It is often seen after the age of 40. Bone Tumors/Metastases indicates that the existing cancer is advanced. These patients should be evaluated in a multidisciplinary fashion (oncology, pathology, radiology, nuclear medicine, and orthopedic oncology).
In recent years, in parallel with the development of cancer therapies, the incidence of metastatic bone cancer has increased as life expectancy has increased. Bone is the third most common site of Tumors/Metastases after lung and liver. Depending on the type of cancer, 20-70% of all cancers (average: 50%) metastasize to bone.
- What are the symptoms of bone metastases? With which complaints do patients consult a physician?
Patients with bone metastases can present to the clinic in many different ways. It is usually detected during routine screening of the cancer patient. Also, some patients are diagnosed with direct bone metastases despite having no history of cancer. It can also be a finding that appears years after a cancer has been treated.
Patients with bone metastases often present to the physician with pain. Typically, the pain is present at rest and increases in intensity over time. The patient may wake at night because of the pain and may not benefit from standard pain medications. Rarely (10-30%), the patient comes to the emergency room with a fracture caused by the Tumors/Metastases weakening the bone.
Numbness, tingling and weakness in the arms or legs may occur due to spinal cord or nerve root compression in patients with vertebral bone metastases. Partial or complete paralysis may develop in case of severe spinal cord compression, especially after collapse due to fracture of the vertebral bone.
- Where is it most common?
Bone metastases can develop in any bone but are most common in the spine, pelvis, femur and humerus. Metastases can be single or multiple.
- Which cancers metastasize to the bone?
All cancers can metastasize to bone, but breast, prostate, lung, kidney, and thyroid cancers are the most common. This is because these cancers are more common in the population and patients with these cancers have a longer life expectancy.
- How is it diagnosed?
The diagnosis of bone metastases is critical, particularly in determining that the tumors do not originate from the bone itself and that they do not originate from a site other than the patient’s existing tumor. Failure to do so could lead to irreversible errors that could have a serious negative impact on the patient’s life. For this purpose, a biopsy may be necessary in some cases, after a detailed review of the patient’s history and physical examination, as well as the necessary radiologic studies.
A two-dimensional x-ray of the entire affected bone is the most basic examination. Although tomography gives a better idea of bone destruction, patients with metastases of unknown origin will have lung and abdominal tomography to try to identify the cancer focus. MRI with medication is the best method for evaluating soft tissue.
Tumor markers are requested as a laboratory test if we suspect Tumors/Metastases in bone lesions detected especially in patients over 40 years of age.
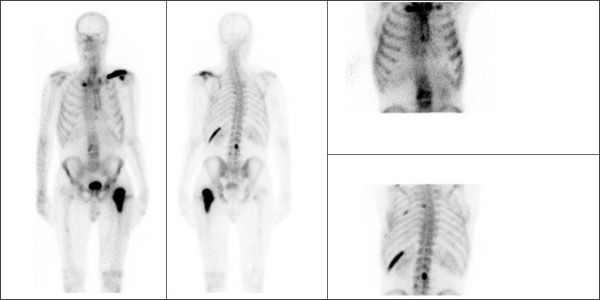
If the patient does not have a history of cancer, or if a nuclear medicine scan (PET_CT or scintigraphy) of a patient with a history of cancer shows a single bone involvement, a biopsy is necessary.
However, in 3-4% of patients, the origin of the tumor may not be identified.
- How are bone metastases treated?
The goal of treating bone metastases is to reduce pain, prevent fractures, and improve the patient’s function/quality of life. The type and extent of the tumor, the size of bone destruction, the response of the tumor to radiation therapy and chemotherapy, the general condition and life expectancy of the patient are the main factors in deciding the treatment. Treatment can be divided into three main categories such as medical (bone-strengthening bisphosphonates, chemotherapy, hormonotherapy, smart drugs) radiotherapy, and surgical. Surgical treatment is used primarily in the presence or risk of fracture. Depending on the patient’s condition, closed (minimally invasive) or open methods may be preferred.
Early diagnosis and intervention is critical, as fracture development due to bone Tumors/Metastases will negatively impact the patient’s life expectancy. Intervention before fracture development reduces the risk of surgery, accelerates the patient’s return to daily activities, and reduces the need for additional surgery. In cases of fractures due to bone metastases, fixation (nail or plate) may be used or the tumor bone may be removed and replaced with a prosthesis. The patient should be carefully evaluated before making this decision. The method used should last for the remainder of the patient’s life and should not require reoperation.
The most common procedure for metastases in the spine is cementing (vertebroplasty). This procedure can be performed under local anesthesia and in a single day. Rapid and effective pain relief can be achieved. The weakened bone is strengthened and collapse is prevented.
- What are the newest methods of treatment in recent years?
The most recent methods in the treatment of bone metastases are image-guided (tomography, mobile x-ray) and closed procedures of burning (radiofrequency ablation, microwave ablation) and freezing (cryoablation). Of these methods, radiofrequency ablation is the most commonly used.
Radiofrequency ablation (RFA) is the process of burning the focus of a tumor at a high temperature under tomography and anesthesia. It can be safely applied to many bones, including the spine. It is an effective method with low risk and quick results. Its additional advantage is that it can be applied to bone metastases that are resistant to radiotherapy or that have recurred after radiotherapy. In certain patients, cementation can be safely applied from the same access site after the tumor has been burned with radiofrequency ablation.
