GIANT CELL TUMOR OF BONE – OSTEOCLASTOMA
- Hits: 753
The exact cause is unknown and it is also called osteoclastoma. It is a benign but aggressive tumor of the bone. What is meant by aggressive is that it causes destruction in the bone and tends to come back after surgery.
It usually occurs between the ages of 20 and 40. It is slightly more common in women.
Patients consult a physician with complaints of pain and swelling. Complaints usually last for 2-3 months. Patients rarely (<10%) present to the physician with a fracture due to weakening of the bone by the tumor.
Neurological symptoms (numbness, tingling, weakness) may develop in spinal localizations.
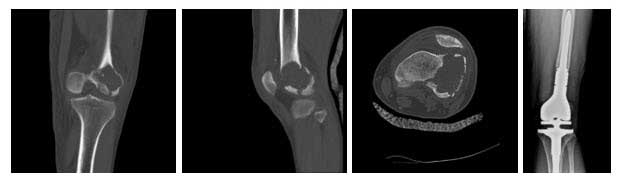
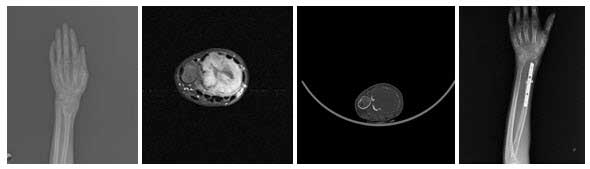
It is most commonly located around the knee (distal femur, proximal tibia) and at the ends of the shoulder (proximal humerus) and wrist (distal radius). In the spine, it is most commonly found in the coccyx (sacrum).
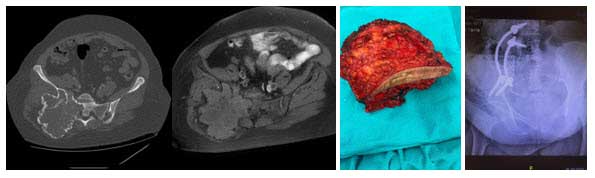
Radiographs show destruction of the outer part of the bone near the joint and usually look like a lytic lesion with indistinct borders.
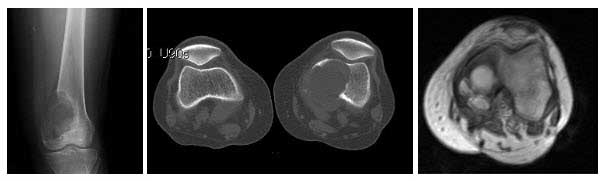
Tomography shows the bone destruction more clearly in three dimensions.
MRI shows the soft tissue component and is helpful in the differential diagnosis. It also guides surgical planning.
A biopsy must be performed for diagnosis. The biopsy is usually performed as a closed needle biopsy under anesthesia. It is important that the physician performing the biopsy is an orthopedic oncologist who deals with bone and soft tissue tumors, and that the pathologist who evaluates the biopsy sample is experienced in this area.
Less than 1% of cases are multifocal. Bone scintigraphy may be performed in appropriate cases to detect this.
The differential diagnosis should include chondroblastoma due to epiphyseal location, aneurysmal bone cyst due to lytic appearance, and telangiectatic osteosarcoma.
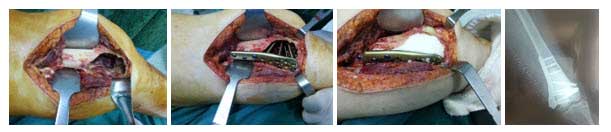
Treatment involves clean removal of the tumor and filling of the cavity with bone graft or cement (often). Bone cement has the advantage of mechanical, cost, ease of recurrence follow-up and the ability to burn residual tumor cells with the heat it emits as it freezes.
To reduce the possibility of recurrence, we perform aggressive curettage with some chemical agents (phenol, alcohol, argon cautery, liquid nitrogen, hydrogen peroxide, etc.), which we call burr and adjuvant after curettage. The possibility of recurrence is high in cases without aggressive curettage. Because of the high recurrence rate of this tumor, it is recommended that the treatment be performed by an orthopedic oncologist who specializes in bone and soft tissue tumors.
In cases of giant cell tumor of the fibula, the tumor bone may be completely removed and left free.
