EWING SARCOMA
- Hits: 1225
Ewing sarcoma is a small round cell malignant tumor of bone. It occurs in 3-4 patients per million per year. Ewing sarcoma often occurs in young patients (<20 years) and is most commonly found in the diaphysis of long bones (femur, humerus, etc.), pelvis, and scapula.
Patients with Ewing sarcoma often present with pain and swelling. The pain is deep and sharp. The pain may increase over time, become severe, persist at rest, and not respond adequately to pain medications. Attributing the cause of the pain to previous trauma may delay diagnosis. Rarely (10%), patients may present with a pathologic fracture due to tumor-induced bone destruction. In this group of patients, general symptoms such as fever and weight loss (often in metastatic patients) and increased temperature at the site of the tumor (may be confused with osteomyelitis) may develop.
Laboratory tests may show elevated white blood cell count, sediment, and CRP (may be confused with osteomyelitis). In addition, alkaline phosphatase and lactic dehydrogenase may be elevated (related to prognosis).
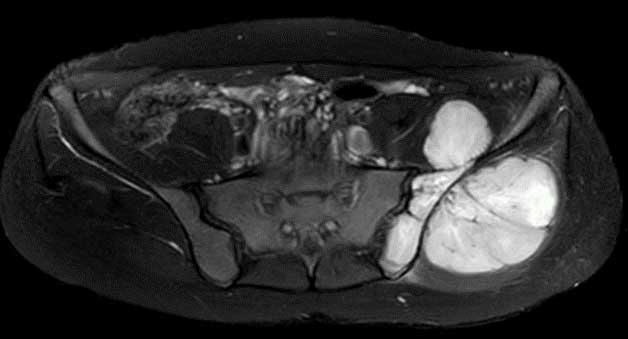
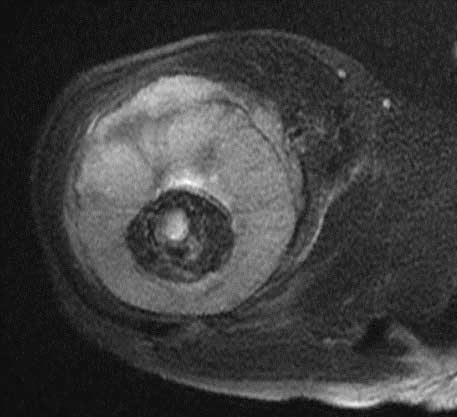
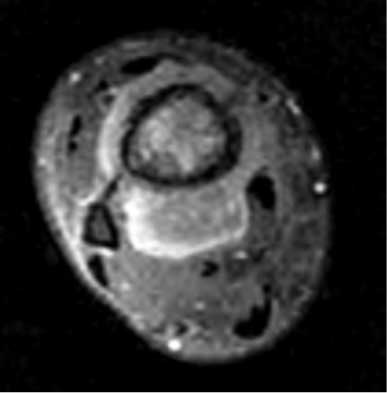
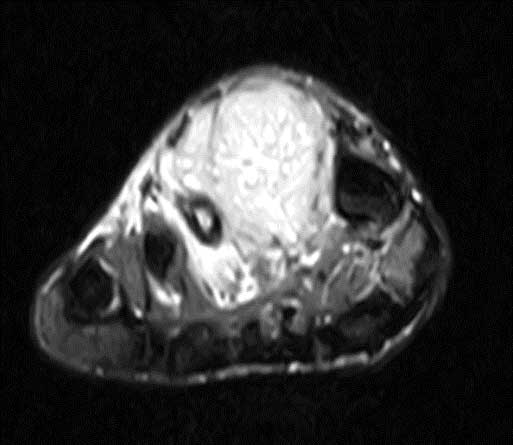
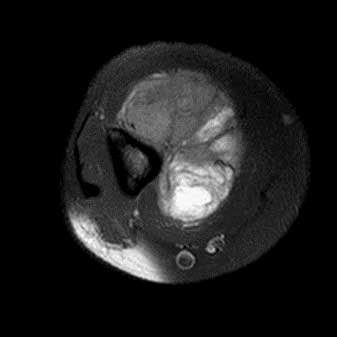
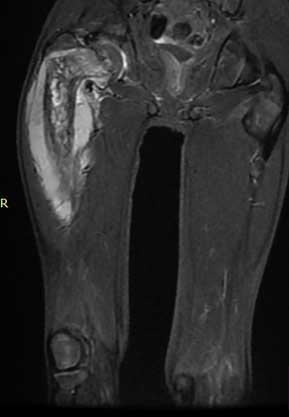
Radiologic evaluation of patients with Ewing sarcoma should begin with direct radiography (x-ray). X-rays provide a two-way view of the entire bone involved. We can get a lot of valuable information (which bone and where the tumor is in the bone, the destruction of the bone and the reaction/periosteal reaction of the bone, the content of the tumor). Permeative bone destruction and onion-skin periosteal reaction are typical findings. In the cortex, a saucer-shaped external to internal recession is a typical finding. In this tumor, a very large soft tissue mass may be seen in association with bone destruction. Contrast-enhanced magnetic resonance imaging gives us detailed information, especially about the soft tissue component of the tumor. We also use it to determine the boundaries of the tumor, its proximity to major vessels and nerves, and the tumor's response to chemotherapy. It also helps us plan surgery.
Ewing sarcoma is diagnosed by biopsy after clinical, radiologic, and laboratory evaluation. Although the biopsy procedure is usually closed using special needles, open biopsy may rarely be necessary. It is important that the physician performing the biopsy be an orthopedic oncologist who specializes in bone and soft tissue tumor surgery and that the microscopic examination be performed by a physician who specializes in bone and soft tissue pathology. Osteomyelitis and eosinophilic granuloma should be considered in the differential diagnosis. The interval between the onset of the disease and diagnosis has been reported to be up to one year. The patient diagnosed with Ewing sarcoma is evaluated for staging. This includes lung and abdominal tomography and whole-body bone scintigraphy or PET_CT. Metastases are found in 25% of patients at the time of diagnosis. Metastases are hematogenous, most commonly to the lungs and rarely to other bones.
In patients without metastases, the average 5-year survival rate is 60-75%. Unfortunately, this rate is much lower in the presence of poor prognostic factors (pelvic/spine location, initial tumor size >10 cm, presence of metastases at diagnosis, poor response to neoadjuvant chemotherapy, and disease recurrence).
The treatment scheme for Ewing sarcoma is neoadjuvant chemotherapy+surgery (wide resection and reconstruction)+adjuvant chemotherapy. Neoadjuvant chemotherapy is usually given for 4-6 cycles. Surgery is then planned using contrast-enhanced MRI and the tumor is removed cleanly with wide margins. The tumor that is not removed cleanly with wide margins has a nearly one hundred percent recurrence rate and is prone to metastasis. For this reason, it is important that the surgeon performing the surgery is an orthopedic oncologist with experience in this area. The gap is reconstructed using biological (reconstruction, fibula, allograft, etc.) or non-biological (prosthesis) methods. Postoperative treatment is completed in one year with adjuvant chemotherapy. Ewing sarcoma is sensitive to radiotherapy, but it is not routinely used in all patients. It is used in the adjuvant setting especially in tumors that respond poorly to chemotherapy and are difficult to remove cleanly by surgery. In addition, radiotherapy is used for definitive purposes in tumors that are metastatic at the time of diagnosis and cannot be removed by surgery.
Patients should be followed regularly for many years after surgery, especially for recurrence and metastasis.
