DESMOID TUMOR - AGGRESSIVE FIBROMATOSIS
- Hits: 2027
It is also called aggressive fibromatosis. The exact cause is unknown, but in some cases it has been associated with estrogen and trauma. Genetic background (familial adenomatous polyposis, Gardner syndrome) may be associated. Patients should be screened for this (family history of colon cancer) and colonoscopy should be performed in appropriate cases.
The incidence is 2-4 per million people per year.
They are mainly located intra-abdominally and extra-abdominally. In the extremities, they are most commonly found around the shoulders and hips/thighs.
It is a benign tumor, but it is locally aggressive, which means that it can cause destruction in the area where it is located and is characterized by frequent recurrence. Localization to the extremities can result in severe disability and loss of limbs. Intra-abdominal tumors can be life threatening.
The natural history of the disease is not fully understood and the ideal treatment has not been fully established.
It is most common in women between the ages of 15 and 40.
Patients often present to the physician with a hard, painless, nonmobile, deep mass that has been present for a long time.
Physical examination reveals a firm and immobile mass. Skin deformity may be noted.
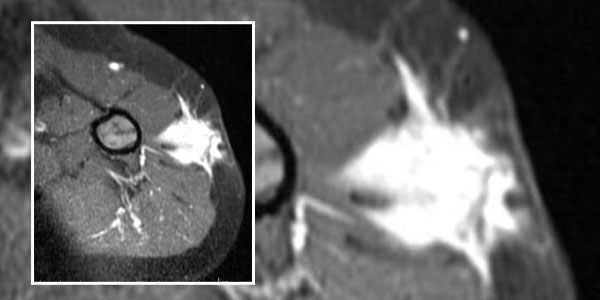
MRI is the most useful imaging modality for diagnosis. It guides treatment planning by showing the location and extent of the tumor. It is also used for follow-up. They grow in the direction of the muscle on which they are located. They can cause destruction in the surrounding bone.
Definitive diagnosis is made by biopsy after clinical and radiologic evaluation. The biopsy is usually performed under local anesthesia and closed with special needles. It is important that the physician performing the biopsy and evaluating the samples is experienced in this area.
There is no definitive treatment. Not every diagnosed desmoid tumor will be removed surgically. Some cases can be followed and the tumor size may remain constant or even decrease. Patients may be given NSAIDs during follow-up. Surgical treatment can be used especially in symptomatic patients with mass effect and compression of critical vascular and nerve structures. In surgical treatment, wide resection should be performed whenever possible. However, clean removal of the tumor with wide margins does not guarantee that the tumor will not recur.
Recurrence rates of up to 50-70% have been reported after surgery. The recurrence rate is high in young patients and in patients without adequate resection.
Radiotherapy, chemotherapy, hormonotrapy or targeted therapies can be applied especially in cases of recurrence and in cases where the tumor cannot be completely removed. Today, Glivec with the active ingredient Imatinib and Nexavar with the active ingredient Sorafenib are the most preferred drugs for treatment.