ANEURYSMAL BONE CYST
- Hits: 1414
An aneurysmal bone cyst is not a real tumour. A bone cyst is an aggressive lesion. In other words, it can damage the bone and may come back after surgery.
In 70% of cases, an aneurysmal bone cyst is seen on its own. 30% of cases are associated with other tumours (giant cell tumour, fibrous dysplasia, etc.).
Aneurysmal bone cysts are more common in women under the age of 30. Patients often present with pain and swelling. Neurological symptoms (numbness, tingling, weakness) may develop in vertebral involvement. Rarely, a pathological fracture may occur due to bone destruction.
An aneurysmal bone cyst is usually located near the tip of a long bone (metaphysis-diaphysis). In patients with incomplete growth plate closure, it may show a transition from metaphysis to epiphysis. It may also be intracortical and subperiosteal. Solid aneurysmal bone cyst is a rare presentation.
Aneurysmal bone cysts involve the posterior part of the spinal bones in 15-20% of cases. Pelvic localization is rare.
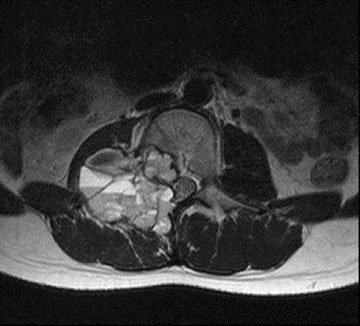
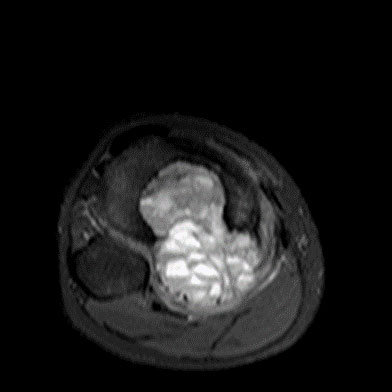
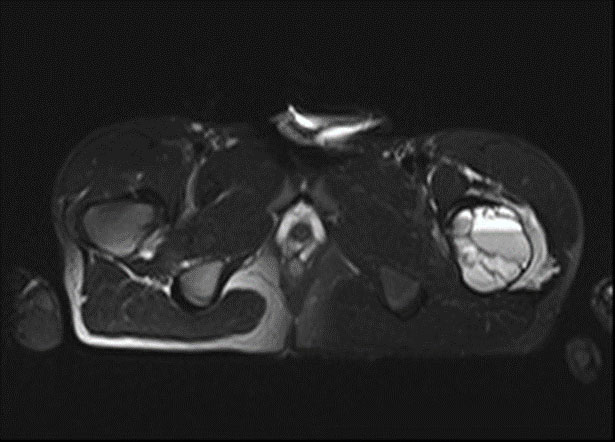
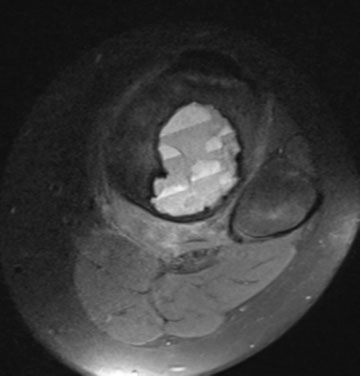
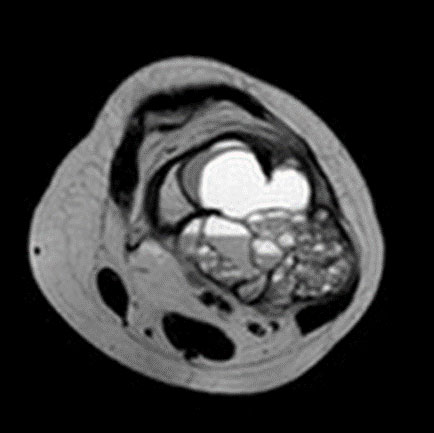
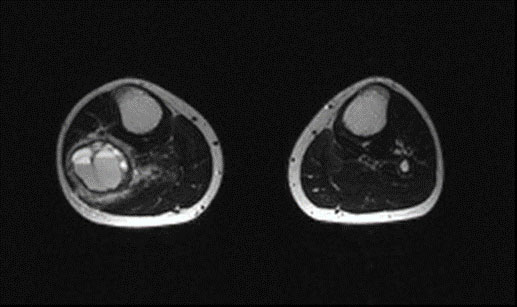
An aneurysmal bone cyst is seen on X-ray as a lytic lesion that expands and thins (destroys) the outer part of the bone (cortex) and is often eccentric. Fine septa and trabeculations are seen within the lesion. CT scans show bone destruction more clearly and are particularly helpful in vertebral and pelvic localization. On MRI, fluid-fluid levels are the typical finding and soft tissue involvement, which is rare, can be demonstrated.
The diagnosis of aneurysmal bone cyst is confirmed by biopsy after clinical and radiologic evaluation. The biopsy is often performed using a closed procedure with special needles. It is important that the physician performing the biopsy is an orthopedic oncologist who deals with bone and soft tissue tumors, and that the pathologist evaluating the biopsy specimen is experienced in this area. The differential diagnosis should include simple bone cyst, giant cell tumor, and telangiectatic osteosarcoma (diagnosis must be confirmed by biopsy).
In the treatment of aneurysmal bone cysts, grafting or cementation is usually performed after curettage. To reduce the recurrence rate (14-34%), burr, cautery, phenol or alcohol application (aggressive curettage) is recommended after rough curettage. In cases without aggressive curettage, the recurrence rate is high. It is important that the treatment be performed by an orthopedic oncologist with expertise in bone and soft tissue tumors. In selected cases, intralesional injection into the cyst (doxycycline, alcohol, etc.) may be used.
Since the aneurysmal bone cyst is a bleeding lesion, embolization (blocking the main vessels feeding the cyst with angiography) may be used to reduce bleeding during surgery, especially in vertebral and pelvic localizations.
The recurrence rate of aneurysmal bone cysts is 14-34% and most commonly occurs within the first 2 years. The risk of recurrence is high in patients under fifteen years of age, aggressive lesions, and inadequate curettage.
Patients should be followed at regular intervals for a long time to assess the risk of recurrence.
