EPITHELIOID SARCOMA
- Hits: 8786
Epithelioid sarcoma is a very rare (less than 1% of all soft tissue sarcomas) malignant soft tissue tumor. Epithelioid sarcoma most commonly affects young adults (20-40 years old) and is slightly more common in men.
Epithelioid sarcoma has an aggressive course, which means there is a high risk of recurrence after surgery and a high risk of spreading to other parts of the body (often lymph nodes and lungs). The average risk of recurrence after surgery is reported to be 50% (30-70) and the risk of metastasis is 40%. About half of recurrent tumors are reported to require amputation. There is also a risk of recurrence in patients who initially underwent amputation.
Because epithelioid sarcoma is slow-growing and usually painless, the average time from onset to diagnosis is 10 (9-30) months. One third of patients have symptoms for more than two years.
Due to the delay in diagnosis of epithelioid sarcoma, lymph node metastases are detected in approximately 1/3 of patients and lung metastases in 1/4 of patients at the time of initial admission.
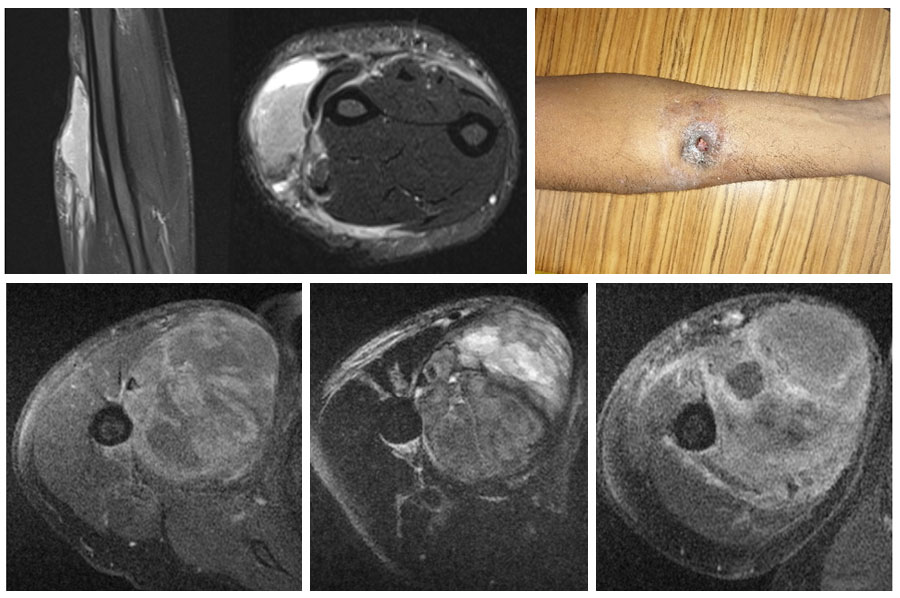
Epithelioid sarcoma can be divided into two main groups. The distal type is localized under the skin in the lower parts of the knee and elbow at a younger age. In a short time (2-3 months), they may break through the skin and ulcerate (12%). In the proximal type, they are located around the shoulder and trunk in the upper extremity and around the thigh and groin in the lower extremity. They are more deeply located and larger in size.
Physical examination usually reveals a painless, firm mass.
The borders of the mass may not be clear on MRI and may appear as multiple foci. Neighboring vessels, nerves, and bone may be surrounded by the tumor. Calcification (ossification) may be seen within the tumor. Hemorrhage and necrosis may be present, especially in large tumors.
The diagnosis of epithelioid sarcoma is confirmed with a biopsy after physical examination and imaging studies have been completed. The biopsy is often performed using a closed procedure with special needles. It is important that the physician who performs the biopsy is an orthopedic oncologist who specializes in bone and soft tissue tumors, and that the pathologist who evaluates the biopsy sample is experienced in this field. The pathology may classify the tumor as angiomatoid, large cell/rhabdoid, or fibroma-like.
After the diagnosis of epithelioid sarcoma, PET-CT or tomography (chest, abdomen, and pelvis) is performed for grading. The need for regional lymph node biopsy has not been fully established.
The primary treatment for epithelioid sarcoma is removal of the tumor with clean margins (wide resection). The tumor that is not removed cleanly with wide margins has a nearly one hundred percent recurrence rate and is prone to metastasis. For this reason, it is important that the surgeon performing the surgery is an orthopedic oncologist with experience in this area.
Adding radiotherapy (high dose and large area) to surgical treatment before or after surgery reduces the chance of tumor recurrence. Therefore, surgery with radiotherapy is the standard of care.
In patients with epithelioid sarcoma, systemic chemotherapy is recommended for locally advanced or metastatic cases. Doxorubicin+ifosfamide, gemcitabine+docetaxel, pazopanib and tazemetostat are among the chemotherapy drugs used for this purpose.
The average 5-year survival of patients with epithelioid sarcoma is 70% for patients with local disease and 50% for patients with regional lymph node involvement. In patients with pulmonary metastases, the one-year survival rate is 50% and the five-year survival rate is unfortunately close to zero.
The prognosis is worse in the presence of tumor diameter >5cm, regional lymphadenopathy, vascular invasion, necrosis rate >30%, local symptoms, positive surgical margins and metastases.
