ADAMANTINOMA
- Hits: 734
It is a rare malignant tumor of bone (less than 1% of malignant tumors of bone origin). It is a low-grade, slow-growing tumor that rarely metastasizes to other organs (especially the lungs).
It is not clear from which tissue the tumor originates. It contains various tissue components (epithelial, endothelial, synovial).
Although adamantinoma can be seen at any age, it is more common between the ages of 10-30 in females and 30-50 in males, and we see it slightly more frequently in males.
It is often (80-85%) localized in the middle region (diaphysis) of the tibia. Very rarely, the adjacent bone (fibula) may also be involved. Adamantinomas of the arm (humerus, ulna, radius) and thigh (femur) have also been reported.
Because the tumor grows slowly, it takes a long time for patients to experience symptoms. Pain and associated swelling are the most common complaints. Approximately one in four patients may develop a pathologic (abnormal) fracture due to weakness in the bone where the tumor is located.
Clinical examination may reveal local tenderness, swelling, and deformity (especially curvature of the tibia - bowing) in the bone where the tumor is located.
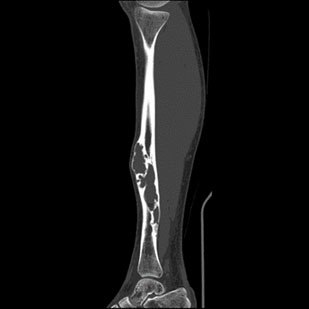
The first step in the radiologic evaluation is direct radiography. The typical finding is a “soap bubble” appearance in the central region of the bone with clear borders in the outer part and lytic and sclerotic components in the inner part. Rarely, destruction of the outer shell (cortex) of the bone may be seen.
Computed tomography is particularly useful in detecting cortical destruction, the presence of fractures, and lung metastases.
Magnetic resonance imaging (MRI) is used in the differential diagnosis of other tumors, intraosseous spread of the tumor, and very rarely to detect a soft tissue component accompanying the tumor in the bone.
Increased involvement is detected in all three phases of bone scintigraphy.
The diagnosis is made by biopsy after clinical and radiologic evaluation. The biopsy is usually performed as a closed needle biopsy. It is important that the physician who performs the biopsy is specialized in orthopedic oncology. It is also recommended that the pathologist who will examine the biopsy material be experienced in bone and soft tissue. There are two pathologic types of adamantinoma. The classic type occurs in patients over the age of twenty and is more aggressive. Differentiated adamantinoma (osteofibrous dysplasia-like adamantinoma, juvenile intracortical adamantinoma) often occurs in patients under the age of twenty and has a more benign course. Recently, Ewing-like adamantinoma has also been described.
Osteofibrous dysplasia should be considered in the differential diagnosis. Osteofibrous dysplasia is usually located at the end of the bone and does not spread into the bone. It is most common in children under the age of 10.
Because adamantinoma is a low-grade tumor, it is resistant to chemotherapy and radiotherapy. Therefore, the main treatment is surgery. The tumor should be surgically removed in one piece with clean margins. The tumor that is not removed cleanly with wide margins has a nearly one hundred percent recurrence rate and is prone to metastasis. For this reason, it is important that the surgeon performing the surgery is an orthopedic oncologist with experience in this area.
The removed bone can be replaced with a fibula taken from the opposite leg alone, or it can be combined with the salvage of the removed bone (liquid nitrogen or radiotherapy). The other option is tumor prosthesis.
The prognosis of the tumor removed with clean margins is very good compared to other malignant bone tumors. However, the patient should be followed regularly for many years for recurrence and metastasis.
Radiotherapy and chemotherapy may be used in patients with metastatic adamantinoma.
