RECONSTRUCTION OF THE CAVITY AFTER TUMOR REMOVAL IN BONE TUMOR SURGERY
- Hits: 1223
The cavity left after surgical removal of bone tumors can be reconstructed/filled using various methods.
Benign bone tumors
For benign bone tumors, we often use bone graft (autograft, which is taken from the patient, often from the pelvis), allograft, which is taken from the cadaver and made ready for use after special sterilization procedures, or synthetic (tricalcium phosphate, etc.) or bone cement.
The advantages of autografting are that there is no additional cost, no tissue compatibility problems, and no risk of disease, but there is a risk of morbidity (pain, infection, hematoma, nerve damage, etc.) in the area where the graft is harvested, and there are limitations in harvesting.
After filling the cavity with these two methods, the bone is mechanically supported with implants (often plates), depending on the location of the tumor and the damage it has caused to the bone.
Although these two methods have their advantages and disadvantages, there is no clear superiority, and the two methods can rarely be combined.
We prefer to use bone grafts especially in patients who have not completed the growth phase. The advantage is that it is biologic and compatible with the host bone in the area where it is placed. The disadvantage is that it takes time for union and become load bearing.
The advantage of bone cement is that it kills tumor cells with its temperature effect and facilitates recurrence monitoring. It also allows early mobilization of the patient by providing fast and strong mechanical support. We generally prefer it in patients whose growth process has been completed.
Malignant bone tumors
In malignant bone tumors, the cavity is larger and is reconstructed by two main methods, biological or non-biological. Both methods have different applications and have advantages and disadvantages.
In addition to life expectancy, the location of the tumor in the bone is important in deciding on reconstruction. If the tumor is located in the joint or near the joint, the prosthesis will be used; if the tumor is located in the middle part of the bone, biological methods will be used.
Biologic methods are often preferred in patients with incomplete growth. The most commonly used method is what we call the vascularized fibula. The main advantage is that it offers more permanent solutions in the long term. For this reason, biological reconstructions are our first choice in patients with a long life expectancy.
The vascularized fibula can be used alone or in combination with salvaged bone (the tumor bone is removed, the soft tissue portion is scraped off, exposed to liquid nitrogen (20 minutes) or radiation (50-60gy), and then re-inserted) or allograft (taken from a cadaver and subjected to certain sterilization procedures before it is ready for use). This increases stability and allows early loading. It is also often supported by plates to increase stability. As the name suggests, its main advantages are that it is biological and compatible with the bone in the area where it is used. Its advantage is that it remodels under load and becomes thicker than the size of the bone in which it is placed and becomes suitable for loading. Union and functional results are good. However, there are rare risks of nonunion and fracture. There is a risk of nerve damage and loss of strength in the leg. It takes time to become weight bearing. There is also microsurgical experience and a long learning process.
As a biologic method, salvaged bone or massive allograft can be used alone or in combination with vascularized fibula as mentioned above. Using them alone has a higher risk of non-union, resorption (loss of original structure) and infection. The combination with vascularized fibula (called composite graft and it combines the mechanical strength of the allograft with the biological effect of the vascularized fibula) provides an advantage in terms of reducing these risks. Massive allograft application is rarely preferred in our country due to availability problems, very high cost and adaptation problems. Salvaged bone does not have the same cost and adaptation problems. However, because not all of the removed tumor bone is sent for pathologic examination, evaluation of chemotherapy response (necrosis rate) and surgical margin may be inadequate. In addition, this method is not suitable if there is severe bone loss due to the tumor.
Another biologic method is external fixation (monolateral or ilizarow), which involves closing the gap by moving the adjacent bone segment. The disadvantages of this method are that it is uncomfortable, there is a risk of nonunion, infection and it requires a long time to complete the treatment (delaying postoperative chemotherapy or radiotherapy). This method is usually preferred to eliminate the final shortness in patients whose treatment has been completed.
Another method is bone transposition, which is the replacement of the removed tumor bone with the adjacent bone. It is especially applied in areas with double bones such as the forearm and cruris (such as fibula instead of tibia, ulna instead of radius). Successful results can be obtained with these methods.
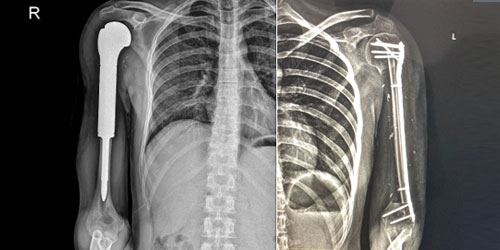
In non-biological methods, tumor resection prosthesis is often used. There are different types depending on the bone where the tumor originates and its location (upper, middle or lower part of the bone). It can be used for malignant tumors that originate from the bone itself, often called primary bone cancer, as well as for bone metastases and benign bone tumors that cause severe damage to the bone (locally aggressive). These prostheses can be customized in size and length (modular). They are usually made of titanium. Rarely, a custom-made prosthesis can be made, but this is time-consuming (6 weeks on average) and expensive. Extendable prostheses are the other option, especially in young patients with incomplete growth, but are similarly costly and have a higher risk of infection. They can be used with or without cement for bone fixation. The advantage is that they provide strong mechanical support and allow early weight bearing. Disadvantages include wear or loosening over time (especially wear of the joint spacer, called polyethylene, and loosening from where it is attached to the bone), fracture, and infection. To reduce the risk of infection, the focus is on reducing dead space and good soft tissue coverage. Another problem is metallosis, the build-up of very small fragments in the joint due to wear and tear.
In very rare cases, we use a combination of a tumor resection prosthesis with a massive allograft or salvaged bone to increase the bone attachment surface of the prosthesis and increase the bone stock for future revision.
